“It is very important that the kids feel involved!”
A Q&A with Dr. Laurence E. Mermelstein, M.D, on the importance of a good patient-doctor relationship in pediatric scoliosis patients
As one of the leading experts in managing the care and treatment of pediatric scoliosis patients and as an active member of the premier Scoliosis Research Society, Dr. Mermelstein’s expertise has helped countless patients, both pediatric and adult, improve their quality of life.
In the Q&A below, Dr. Mermelstein gives answers to parents’ pressing questions and explains why it is so important that children are involved in decisions regarding their care.
Pediatric Patient-Doctor Relationships
What should parents look for in an orthopedic surgeon when their child has scoliosis?
Dr. Mermelstein: I would recommend that they look for an orthopedic spine surgeon who has experience with pediatric deformity surgery. The surgeon should be familiar with ALL types of surgical approaches so that he can discuss ALL different options with equal experience. Preferably, the surgeon should have a practice specializing spine surgery (as opposed to a surgeon taking care of a mix of spine and non-spinal issues).
I notice that you will speak directly to your young patients. Can you tell us why you think that is important?
Dr. Mermelstein: The kids are the patients here. They need to take ownership of the decisions, whether they want to or not. Of course, the heavy lifting when it comes to decisions is still done between the parents and myself, but it is very important that the kids feel involved. Otherwise, I might as well be doing veterinary surgery. When the kids have involvement in the decisions, they do not feel as powerless and they are involved in their recovery—and results are better.
What do you recommend to a parent/patient when they don’t feel that their medical provider is listening or addressing their concerns?
Dr. Mermelstein: I would ask them if there was another time or forum outside of the traditional office visit where they could communicate. Email has been helpful in getting extra time and answers. Phone conferences after hours are helpful as well. Sometimes the doctor can feel very rushed and strained in the middle of clinic hours. They may be able to listen and respond better in another format. If that doesn’t work, you may need to seek answers elsewhere.
Is it possible that although it’s called “adolescent” scoliosis that it may have existed undetected years before? Is it just the adolescent growth spurt that makes scoliosis more apparent?
Dr. Mermelstein: By definition, idiopathic scoliosis is not present at birth. Again by definition, it is first detected in kids, ten- to sixteen- years of age. If the curve is seen before ten years of age, it is termed “juvenile” or “early onset” idiopathic scoliosis. The earlier that the curve presents, the more likely the curve will progress. It is with the rapid growth acceleration that occurs with puberty that the magnitudes of these curves sometimes increase rapidly.
Other than the classic rib “hump” upon bending, what are some of the other earlier common signs of idiopathic scoliosis that parents can be aware of?
Dr. Mermelstein: One can see shoulder asymmetry, elevation, etc. Look for scapula asymmetry, waist asymmetry, chest, or sternal asymmetry. Forward bending highlights the ROTATIONAL component of scoliosis in the thoracic (ribs) and lumbar (flanks).
What do you do when a child complains of pain?
Dr. Mermelstein: There usually is no pain associated with idiopathic scoliosis, but if a child complains I will assess the problem to make sure nothing more serious is going on. If everything is fine, that child might benefit from some physical therapy. If pain continues, an MRI may be indicated.
Bracing
Do you have a brace of preference? If yes, which one and why?
Dr. Mermelstein: Over the last 5 -7 years, we have been recommending the Rigo-Cheneau (or modification of) bracing system. Although the definitive studies have yet to be released, the preliminary evidence is that we are getting better correction and ultimate results with this brace – better than the Boston brace, which I used previously. I also continue to use the Charleston bending brace, a night time only brace, in select children with select curves. This has obvious advantages with respect to compliance.
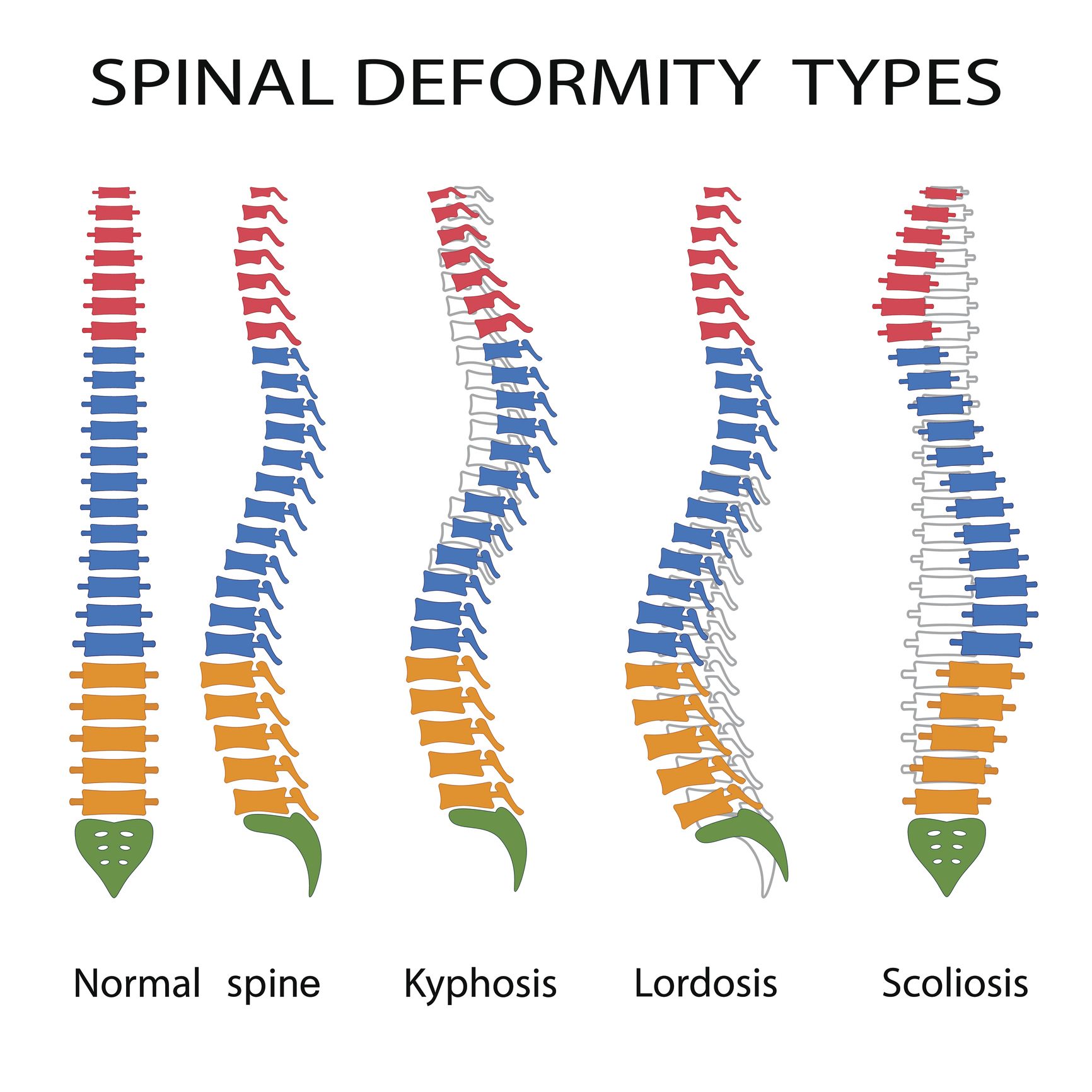
Illustration of spinal deformity types. Kyphosis, lordosis and scoliosis.
Why is there a discrepancy among orthopedic spine surgeons regarding the number of hours for brace wear (sixteen hours versus twenty-three hours)?
Dr. Mermelstein: Research has shown that the more time in the brace, the better. The efficacy is “dose” (time) dependent. To my knowledge, there is no “threshold” time above which it is not helpful or even counter-productive. My experience is that, in kids, we shoot for twenty-three hours a day, realizing the actual time will be much less, accounting for bathing, swimming, sports, and gym class. In dealing with adolescents, I do not give a number of hours to wear the brace. Invariably, this becomes the maximum hours we get and on average, the compliance is much less. I want to avoid having kids “watch the clock” – this puts too much focus on the brace and not enough on the rest of their lives.
If a child had a 20º curve, would you begin bracing as an early intervention?
Dr. Mermelstein: Not usually, I probably would just continue to monitor that child. I don’t like to put a child in a brace any earlier than I have to. If the patient is seventeen years old and four years post-menarche, there are no reasons to brace. However, if there is evidence of family history of scoliosis, I might be more aggressive. If I have an eight-year-old child who has a rather stiff curve, and whose mother and grandmother had surgery on their scoliosis, I would intervene with bracing sooner.
When do you decide your patient needs to go to full-time bracing?
Dr. Mermelstein: I usually will start full-time bracing when the curve reaches 25º and the child still has a lot of growth remaining. If for some reason I’m not sure about the growth remaining, I will send them for a bone age x-ray. The benefit of the wrist film is that it gives you a different angle on their bone age.
What factors do you use to determine when bracing is nearing its end?
Dr. Mermelstein: Bracing is usually completed when a patient is skeletally mature. This is determined in a number of ways, some more complicated than others. Simple methods are a patient’s menstrual history (in girls), their height in comparison to their parents/older siblings, iliac crest growth plates (Risser sign) that is easily seen on xrays of spine. If there is any debate, a “bone age” using x-rays of the left hand can be obtained. The growth plates of the hand are compared to an “atlas” of typical children of a similar “age” and skeletal maturity is assessed. The simplest way, if I have the data, if to look at the growth curve, which I can develop from my chart of height in the office. If a child has not grown in 2 consecutive visits, and other factors as above are in agreement, we can discuss a weaning protocol. This is less true in boys who can have late, unpredictable growth accelerations.
Do you implement a weaning phase for your patients? If yes, please explain.
Dr. Mermelstein: To be clear, just because a child has been diligent at wearing a brace and they hit milestones that say she is skeletally mature, doesn’t mean they discontinue the brace and all is well. It is not uncommon for a child with a curve, which has been well controlled in the brace to demonstrate progression of their curves after they stop the brace (even though they are skeletally mature). Depending on the type of brace and the numbers of hours the brace is being worn, we slowly increase the hours out of the brace and recheck x-rays at subsequent visits. If a curve progresses with decreasing brace wear, we stop the weaning and maintain the bracing time. Sometimes this means we are continuing bracing well after growth has ceased. Depending on the magnitude of the curve when kids reach skeletal maturity, curves can continue to progress as “young adults” when bracing is eventually stopped. In these cases, we discuss surgery to arrest the progression (and correct the curve).
Can curves continue to progress post-bracing? If yes, under what circumstances?
Dr. Mermelstein: Yes. Curves can progress after a brace is worn and growth ceases. I wish I could tell you why this happens in some patients and not in others. Many times, it has to do with the degree the curve winds up in after growth ends. Curves that are close to 40º and above have a higher likelihood of progression into adulthood, than curves less than 30º. That is why surgery is recommended for these larger curves; they do tend to progress, albeit at a slower rate than during puberty.
Do you recommend the Schroth Method as part of your treatment plan today?
Dr. Mermelstein: This approach to scoliosis treatment was developed by Katharina Schroth and further popularized by her daughter Christa. Born in Germany in late 1800s, Katharina Schroth had scoliosis that was unsuccessfully treated with bracing. She developed her own breathing technique and exercises to manage her scoliosis. It is only recently in the last 10 years that this program has been used by Physical therapist in the US. The Schroth therapist focuses on elongating and derotating the scoliotic or kyphotic spine, in an effort to stop/slow curve progression and prevent further spinal deformity. A treatment session typically lasts 45 minutes and encompasses hands-on stretching, passive positioning and active breathing techniques. There are a relatively small number of therapists who provide this treatment, as it requires additional certification and significantly more time. Studies are underway to determine if this approach is able to arrest or reverse the progression of scoliosis.
Surgery
Why does there seem to be discrepancy among surgeons as to what degree to surgically correct scoliosis? Can you describe typical scenarios requiring different recommendations?
Dr. Mermelstein: There is no absolute consensus regarding surgical indications for scoliosis. Indications for surgery are not based on degrees alone, although there is a general number of about 45º, give or take. The goals for surgery are correction, obviously, but equally important is to arrest progression. Not all 40º to 45º curves have the same risk. Thoracic curves are more likely to progress and the younger the patient the more likely surgery is suggested. A curve that is imbalanced is more likely to require surgery. Indications for adult scoliosis surgery are completely different, and more likely to require surgery for pain at a lesser degree magnitude. Different surgeons will be more or less aggressive and they each have their own reasons. It is the same for ALL types of orthopedic surgeries, arthroscopy to joint replacements.
What is an anterior fusion? Can you explain when this would be appropriate and what is entailed?
Dr. Mermelstein: Fusion surgery for scoliosis performed from the side is called an “anterior fusion.” It is most frequently used for primarily lumbar curves. In this surgery, the entire disc is removed and the anterior ligaments released. This may allow for a better correction. Bone graft is put directly in between the vertebrae in the disc spaces. Usually anterior instrumentation is put on the side of the vertebrae holding the correction until fusion is achieved. The advantage of this is that fewer vertebrae can be fused, especially lower down in the spine. Also, a selective lumbar fusion can be done, which is much less surgery. Lumbar and thoracic curves cannot be addressed with this approach at the same time. A separate surgical incision would be needed to address a thoracic curve at the same time; therefore, it is not usually done in double major curves (unless the curves are so stiff that they need an “anterior release”). Disadvantages are that the instrumentation fixation may not be as good anteriorly, as it is with pedicle screws posteriorly.
When making a decision about surgery for a child, what should parents look for in a hospital?
Dr. Mermelstein: The hospital has to be used to handling complex spinal procedures in the operating room with respect to anesthesia, instrumentation, and equipment. Cell Saver® blood scavenging needs to be available. Spinal cord intra-operative monitoring (IOM) needs to be available with staff experienced in these cases. The hospital needs to have a post-operative monitored care environment (ICU or “stepdown”) that is comfortable taking care of spinal surgery patients. It is always helpful to be close to home so that post-operative complications can be handled in a timely fashion. It is nice that the parents can stay with the child as much as they desire (although I do recommend they get some quality sleep at some point!).
What is an intra-operative monitoring system?
Dr. Mermelstein: Intra-operative spinal cord monitoring (IOM) has become the gold standard for monitoring the function of the spinal cord during scoliosis correction surgery. Over the last ten years, the motor and sensory function of the spinal cord can be continuously monitored in real time during the surgery. Electrodes are placed on the patient’s skull and in various muscles in the abdomen and legs. Impulses are sent to the brain and recorded in the muscles and vice versa. Any intra-operative maneuvers or corrections that may impair spinal cord function can be reversed in a timely fashion, thereby, minimizing post-operative deficits. Prior to the advent of IOM, a “wake-up test” was performed after the correction maneuvers and before the wound was closed. The patient was woken up while still on their stomachs during the surgery. If they had trouble moving their feet and legs, a spinal cord injury may be detected.
What are some things that you might recommend a child do prior to surgery to help get the best result?
Dr. Mermelstein: There are many things to do to prepare. Individually, each patient should be in as good physical shape as possible. Maximizing cardiovascular endurance will help in recovery and help minimize pulmonary complications. Skin hygiene is important (an issue in many adolescents). If acne is an issue in the surgical area, this needs to be addressed. Making sure the house is configured for easier recovery is important (make sure everything is on one level, if possible).
Recovery
While in the hospital, how will a parent be able to assess if their child’s pain is being managed effectively?
Dr. Mermelstein: The patient should be able to roll from side to side and be able to get out of bed without a severe amount of pain. Pain cannot be completely eliminated, nor should this be the goal. If a patient is over-medicated, they will be overly sedated, and unable to participate in physical therapy and walking.
How soon after a child’s spinal surgery do you recommend getting out of bed?
Dr. Mermelstein: The next day.
When do you allow your patients to return to gym/sport activities after spinal fusion surgery?
Dr. Mermelstein: Full healing from scoliosis surgery requires full healing of a spinal fusion. Typically, this takes at least 4-6 months, sometimes longer. It also depends on the amount of surgery (how long a fusion) the patient had as well as the type of sport. For any impact activity or activities requiring twisting and lifting, I prefer to wait at least 9 months before clearing for activity.
Long term, are there any activities that could cause pain after spinal fusion surgery? Running, tennis, golf, gymnastics, etc
Dr. Mermelstein: Generally, after a child has healed up 100% from surgery, most activities should be pain free. If a child has a significant amount of lumbar spine fused, she may feel stiff or restricted in their mobility due to loss of motion in the lower back. Because of this, if a child has undergone a significant lumbar fusion, I counsel against activities such as gymnastics and certain types of dancing that require a significant range of motion. Otherwise, I allow kids to go back to almost all types of sports except contact sports (eg. Football, rugby).
Our patients, employees and family are our top priority at Long Island Spine Specialists, P.C.
We ask you to not visit any of our locations if you have symptoms such as fever, sneezing, coughing and possible shortness of breath.
Please cancel your appointment and re-schedule once you are feeling better and are no longer suffering with symptoms.
Only non-symptomatic patients will be seen. No exceptions.
Accompanying family members – including children – are asked to remain in the waiting area and will not be allowed to enter the exam rooms.
During this time of high concern regarding the spread of COVID-19 (Coronavirus) we are taking extra precautions to maintain the highest possible standards of safety and cleanliness. Please be advised that we are carefully following recommendations from both the CDC and WHO and are here to help guide you through this time if needed.
Some steps we are taking to keeping safe:
We know how important cleanliness is and always maintain the highest standards of cleanliness. To further offer you peace of mind, we have increased the frequency of the cleaning of our office.
Rest assured that hand washing is strictly followed. Hand sanitizer is available to all staff and patients.
Additionally, if you have recently traveled to a country with high rates of the coronavirus or have been on a cruise, please reschedule your visit for at least 14 days from your return date. We will gladly accommodate your needs to reschedule. At that time, a telehealth interface can be arranged if necessary.
Find up-to-date and accurate information on the Centers for Disease Control and Prevention (CDC) website and feel free to reach out with questions.
- Your team at Long Island Spine Specialists, P.C.
To learn more about Long Island Spine Specialists – and to discover how we can relieve your pain and help you find an improved quality of life – please contact our office today and schedule a consultation.
Accessibility: If you are vision-impaired or have some other impairment covered by the Americans with Disabilities Act or a similar law, and you wish to discuss potential accommodations related to using this website, please contact our Accessibility Manager at (631) 837-2359.